By GRSM MedicareTeam on November 22, 2019
Rulemaking for Civil Monetary Penalties and regulations believed to promulgate formality to Liability and No-Fault Medicare Set-Asides has been pushed back to December 2019 and February 2020, respectively.
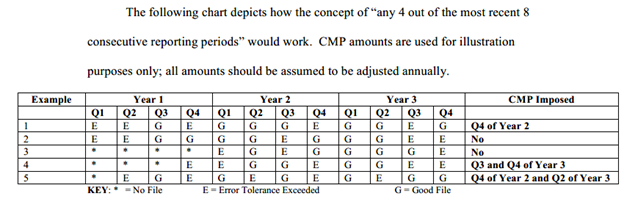
Rules clarifying when and how penalties may be issued for Section 111 Medicare Mandatory Insurer Reporting noncompliance could possibly be issued by year’s end. The industry has been anticipating this rule since the initial $1,000 per day per claim penalty was softened into a discretionary penalty per the SMART Act of 2012, enacted in 2013. The updated notice can be viewed here.
Rulemaking for an LMSA or NFMSA policy no longer appears to be imminent. The last date published was October of 2019, which is now delayed another three months, at least. CMS approached such policymaking in 2012, redacting it in 2014 only to revisit it again in 2016. The industry remains in a holding pattern, which will continue through the first several months of 2020, if not longer. https://www.reginfo.gov/public/do/eAgendaViewRule?pubId=201910&RIN=0938-AT85
The Office of Information and Regulatory Affairs’ (OIRA) Office of Management and Budget (OMB) page shows some changes to the Miscellaneous Medicare Secondary Payer Clarifications and Updates proposed rule. Of note is the priority for this rule, which has been shifted from Economically Significant to Other Significant.
According to the OIRA/OMB Frequently Asked Questions, page, a proposed rule that is Economically Significant can be defined as follows:
“A regulatory action is determined to be “economically significant” if OIRA determines that it is likely to have an annual effect on the economy of $100 million or more or adversely affect in a material way the economy, a sector of the economy, productivity, competition, jobs, the environment, public health or safety, or State, local, or tribal governments or communities. For all “economically significant” regulations, the Executive Order directs agencies to provide (among other things) a more detailed assessment of the likely benefits and costs of the regulatory action, including a quantification of those effects, as well as a similar analysis of potentially effective and reasonably feasible alternatives.”
The term “Significant” is also defined on the OIRA page, and it can be distinguished from Economically Significant status as the proposed rule could:
- Create a serious inconsistency or otherwise interfere with an action taken or planned by another agency;
- Materially alter the budgetary impact of entitlements, grants, user fees, or loan programs or the rights and obligations of recipients thereof; or
- Raise novel legal or policy issues arising out of legal mandates, the President’s priorities, or the principles set forth in this Executive order.
The OIRA page further distinguishes “Significant” status as follows:
The Executive Order requires that significant regulatory actions be reviewed by OIRA before they are published in the Federal Register or otherwise issued to the public. The Executive Order also requires agencies to provide an explanation of the need for the regulatory action and an assessment of potential costs and benefits. OIRA generally designates between 500-700 regulatory actions as significant each year.
Of interest is the bit about the proposed rule raising novel legal or policy issues arising out of legal mandates. Of further interest is the removal of some of the abstract language on the OIRA agenda page, which removes the following part of the rule’s description,
“Currently, Medicare does not provide its beneficiaries with guidance to help them make choices regarding their future medical care expenses when they receive automobile and liability insurance (including self-insurance), no fault insurance, and workers’ compensation settlements, judgments, awards, or payments, and need to satisfy their Medicare Secondary Payer (MSP) obligations.”
This leaves only the following description of the rule in the Abstract: “This proposed rule would ensure that beneficiaries are making the best healthcare choices possible by providing them and their representatives with the opportunity to select an option for meeting future medical obligations that fits their individual circumstances, while also protecting the Medicare Trust Fund.” Essentially, Medicare is no longer indicating that the Beneficiaries do not have guidance about future medical. This could possibly correlate to the prior Medicare Learning Network publications the Agency had disseminated to medical providers, suppliers and facilities. These publications suggested that Medicare Beneficiaries could be billed directly for services if Section 111 reporting was filed, demonstrating a primary payment plan’s availability, with Medicare as a Secondary Payer. The removal of language that there has been no guidance by Medicare could indicate positioning for greater accountability about Medicare Set-Aside usage. This is consistent with recent changes in the Workers’ Compensation Medicare Set-Aside Reference Guide (WCMSA) Version 3.0, which requires a Beneficiary’s acknowledgement of MSA content, intent, submission processes and associated administration within the Consent Form, as of April 1, 2020. See our article on this here.
What has not changed in the Abstract is Medicare’s suggestion that any proposed rule will be voluntary in nature, although the change to “Significant” status broaches the possibility that there could be a policy concern or legal mandate involved.
GRSM’s Medicare Compliance Group will continue to monitor the status of any forthcoming rulemaking.